Get educated
ON PBM ABUSE & OTHER ISSUES
IN PHARMACY

SHINING A LIGHT ON UHG
SHINING A LIGHT ON UHG

HEALTH CARE un-covered’s new Sunlight Report on UnitedHealth Group (UHG) is a first-of-its kind look at the nearly 2,700 acquisitions and internally created subsidiaries that make up UHG, the largest healthcare conglomerate in the world. Using the analysis of publicly available data, the report was designed specifically to help the public more clearly grasp the scope of the company’s reach (and that of others’ like them).
Improving a problem starts by learning about it: where and why it’s happening, who it’s affecting (both positively and negatively), and what’s already (or not) being done about it.
Below you’ll find a collection of educational resources to help you better understand issues currently going on in our industry (and, consequently, our healthcare system at large). We’ll focus primarily on Pharmacy Benefit Manager (PBM) abuse, since the anti-competitive, unethical conduct of these top Fortune 100 companies—the middlemen when it comes to processing prescription claims and some of our nation’s biggest and most profitable companies—is at the heart of why our crumbling healthcare system puts profits over patients, providers, and the entities that help pay for patients’ care (including state and federal governmental programs, such as Medicaid and Medicare).
“Patients go without the services they need
for [PBMs’] greed.”
—John V. Hoeschen, RPh, BSPharm, Owner & Pharmacist of St. Paul Corner Drug

The short story: community-based pharmacy care is dying in our nation… quickly.
The long(er) story: for decades, pharmacies like us have been facing the threat of closure from—and we know it sounds crazy—losing money fulfilling our primary role of filling prescriptions. This is because, in our industry, for-profit insurance companies have been allowed to underpay us (or even take money away) for providing pharmacy care, and this issue exists alongside large-scale anticompetitive practices such as vertical integration and algorithmic price fixing. This has resulted in us “little guys” being forced to bend over backwards to keep our doors open and lights on while operating in an industry that, while tasked with providing essential healthcare, has grown to include something of the wealthiest companies in the world*—wealth that is not, as they’ve worked hard to make others believe, leading to a healthier America. Rather, their unchecked greed is keeping money in their coffers while patients face worsening outcomes and access to healthcare of all kinds while healthcare providers are finding it increasingly difficult to care for patients, whether it’s because they financially can’t afford to, are too burned out from interacting with a crumbling health system on a daily basis, or both.
Local pharmacy, whether chain (e.g., CVS, Walgreens) or independent (like us), has taken a particularly hard hit. Hundreds of independent pharmacies are lost every year, the most of which, unfortunately, have occurred in our home state of Minnesota. To see the impact of pharmacy closures in real time, check out the University of Pittsburgh’s map of US pharmacy closures. Most individuals don’t realize how valuable community-based pharmacies are until they’re living in a pharmacy desert** without access to one; while our primary role has traditionally been filling prescriptions, we also offer to our communities home delivery and/or mailing of both prescriptions and over-the-counter items, Medication Therapy Management (MTM) services, vaccination, access to lifesaving medications like Naloxone and emergency contraception, and more. However, given the current climate, we can guarantee that, once a local pharmacy closes, it won’t be replaced until legislative action and large-scale reform of the insurance industry ensures we’re reimbursed appropriately for the work we do.
Continue reading below to learn more about issues in pharmacy and our favorite educational resources. Once you understand what’s going on and what’s at stake, you can help support the movement by contacting your legislators about state and federal legislative initiatives, sharing your story, and spreading the word!
*The three largest drug wholesalers—AmerisourceBergen, Cardinal Health, and McKesson—Pharmacy Benefit Managers (PBMs)—CVS Caremark, Express Scripts, and OptumRx—and big-box companies that provide pharmacy services—Amazon, Costco, and Walmart—now represent nine of all Fortune 15 companies
**Click here to learn more about this newfound term that, similar to the meaning of a “food desert,” denotes an area where individuals lack adequate access to pharmacy care
Minnesota has endured more pharmacy closures than any other US state
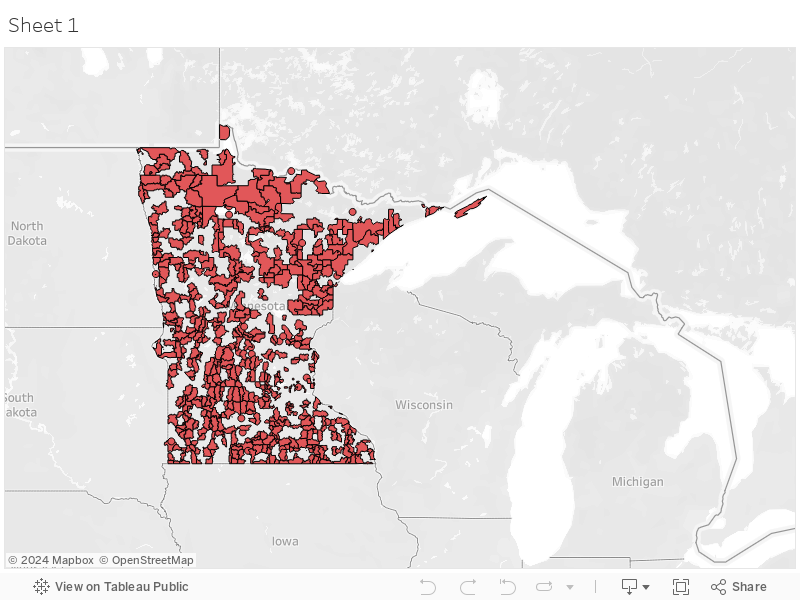
Navigate the interactive map to the left or click below to explore a map of Minnesota’s growing pharmacy deserts.
A 2024 study ranked Minnesota 10th in the nation for the largest proportion of residents living in a pharmacy desert. The data, collected in 2022, showed 7.2% of the state’s total population lacked access to a community pharmacy, (Wittenauer et al., 2024).
Pharmacy Benefit Manager Mafia: The basics
One of the biggest threats to community-based pharmacies like us has been and continues to be the abusive conduct of for-profit insurance companies, especially the PBMs that represent them in the pharmacy arena of healthcare.
What’s a PBM?
Pharmacy Benefit Managers (PBMs) are “companies that manage prescription drug benefits on behalf of health insurers, Medicare Part D drug plans, large employers [who are self-insured], and other payers [such as state Medicaid programs]” (The Commonwealth Fund, 2019). In the American healthcare system, they’re responsible for handling:
The automated processing of Rx claims (i.e., they’re the reason the billing of your prescriptions is increasingly convoluted, putting greater logistical burden on patients, providers, and payers)
Creating the "formulary" of covered drugs for payers (i.e., they’re the reason your medication is covered, your prescription requires a PA, or why you have to take the expensive brand-name version of a medication when a cheaper generic version exists)
Negotiating rebates with drug manufacturers (i.e., they have a financial incentive to create formularies that include those manufacturer’s drugs)
Creating pharmacy networks
Reviewing drug utilization
Managing mail order specialty pharmacies (i.e., they’re the reason that mail order pharmacies are cumbersome to work with, to the point of significantly negatively impacting patients’ care experience (sometimes even in outright unethical ways))
Have you heard of…?
CVS Caremark (owned by CVS Health, which also owns Aetna) | $8.3 billion (twice that of 2022)*
Express Scripts (owned by Cigna) | $7.4 billion (Cigna)
Humana | $2.489 billion
MedImpact (affiliated with Blue Cross Blue Shield, HealthPartners) | Still researching!
OptumRx (owned by UnitedHealth Group) | $22.3 billion* (UnitedHealth Group)
Prime Therapeutics (affiliated with Blue Cross Blue Shield) | Still researching!
*As reported by a third-party source; unable to locate company’s 2023 official financial report
The above listed PBMs are the biggest in the US, with CVS Caremark, Express Scripts, and OptumRx together accounting for about 80% of the entire market. Each company’s annual profits as officially reported for 2023 (listed to the right of their name) highlights just how exorbitant their profits are relative to the pervasive harm they cause on a daily basis, including:
-
Increased difficulty filling your prescriptions due to logistical burdens like Prior Authorizations (PAs), inability to connect with insurance companies via phone, etc.
Being forced to take (and pay for) expensive brand-name medications when a cheaper generic alternative exists (because the generic isn’t included on your plan’s formulary)
Increased difficulty affording your prescriptions
Being forced to change pharmacies (e.g., when patients with a particular health plan are forced to move their medications to a mail order pharmacy, which is considered “patient steering” and is outright illegal)
Increased difficulty accessing pharmacy care as more and more community-based pharmacies close
-
Increased difficulty filling prescriptions due to logistical burdens like PAs, inability to connect with insurance companies via phone, etc.
Decreasing ability to accept a diverse array of insurance plans, which makes us less accessible to our patients (especially those who face financial challenges and MUST use insurance in order to afford their prescriptions)
Inability to keep our businesses financially viable due to under- (or complete lack thereof) reimbursement for the cost of filling prescriptions
Closing our businesses due to employee burnout
-
Increased difficulty prescribing certain medications due to logistical burdens like PAs, inability to connect with insurance companies via phone, etc.
Decreasing ability to accept a diverse array of insurance plans, which makes them less accessible to patients (especially those who face financial challenges and MUST use insurance in order to afford their healthcare)
Inability to keep their businesses financially viable due to under-reimbursement for the cost of providing health services
-
Overpaying for pharmacy services rendered (especially in the cases of Medicaid and Medicare funding, which ALL taxpayers contribute to!)
[PBMs’] business model evolved from a simple data conduit to the most influential player in the prescription drug marketplace. —Todd Stephens, COO of Stephens Pharmacy & Northeast Med-Equip

What’s PBM abuse?
PBM abuse is an umbrella term referring to the various ways in which the PBM industry abuses the American healthcare system and the “3 P’s” within it (patients, providers, and payers) in both ethically questionable and outright illegal ways. This includes:
Inappropriately low or no reimbursement to pharmacies for services provided (dispensing prescriptions, vaccination, etc.)
Since 2007 (when Medicare Part D was created), the retroactive collection of DIR fees ("clawbacks") from pharmacies on all Medicare claims, which have increased 117,000%
In 2023, our pharmacy alone paid around $360,000 in DIR fees, which is equivalent to the annual salary (plus benefits) of 2 full-time pharmacists
Abusive, one-sided contracts with gag clauses that limit pharmacies’ ability to be transparent with patients and provide zero protections for pharmacy providers
Patient steering = illegal practice in which an insurance company/PBM forces a patient to use a particular pharmacy that they own or are affiliated with
Forcing patients to take expensive brand-name medications when a cheaper generic alternative exists… and more!
To make matters worse, all of the above occurs in an industry with little to no transparency, making it incredibly difficult to increase awareness and understanding of this problem while making it easier for PBMs and insurance companies to continue to abuse the system.
On November 1st, 2022, we temporarily stopped taking new patients at St. Paul Corner Drug because we are facing the ever-growing obstacle of losing money performing our primary job: dispensing prescription medications to patients (which is, put simply, due to the misconduct of PBMs). And so, for us, more patients does not lead to positive growth; rather, it simply adds to our already stretched workload in a way that prevents us from providing the safe, efficient care we’re known for, while simultaneously pushing us even further into the “red zone.” This is an obstacle that, no matter how much reinventing we do or creative we get, will remain insurmountable as long as PBMs are allowed to continue legally stealing from patients like you, providers like us, and the payers (such as the state and federal government, in the case of Medicaid and Medicare programs) who help cover the cost of your healthcare. And when providers like us—community-based, independently owned pharmacies—go away in our current environment, it will likely be for good; along with it will be the personalized, hands-on, readily accessible care we provide to American residents.
Every day, people come into our pharmacy and, when they can’t transfer their prescriptions to us or can no longer get their medications and vaccines covered at our pharmacy because of their health insurance plan, ask us what they can do to help. You’ve started just by reading the information on this page! Next, check out the educational resources below to learn more about PBM abuse and let us know if you have any questions; then, head back to our Advocacy page to read about other ways you can help, including contacting your state and federal legislative representatives about ongoing legislative initiatives.
Watch our Nurse, Hildie, present to MNORN about PBM abuse!
Click on the image to the left to access the recording of this presentation, which provides a more in-depth analysis of the various intersecting elements of PBM abuse and touches on action items that concerned individuals can take. Hildie’s presentation slides and a summary handout are also available via this link (her presentation is listed under “January 2024”). Sharing this recording with others—including the lawmakers who represent you at both the state and federal levels—can help them learn, too!

Educational Resources
Our go-to’s
The educational resources below are some of our favorites to refer people to when they’re first learning about Pharmacy Benefit Manager (PBM) abuse and other issues in the pharmaceutical industry.
The Commonwealth Fund | Private foundation dedicated to promoting a high-performing, equitable health care system through supporting independent research on health care issues and making grants to improve health care practice and policy
HEALTH CARE un-covered | Newsletter created by self-proclaimed “reformed insurance propagandist” Wendell Potter to call attention to out-of-control profiteering in US healthcare and what that means to everyday Americans, as well as identify potential solutions
Pharmacists United for Truth & Transparency (PUTT) | Non-profit advocacy organization founded by independent pharmacists and pharmacy owners devoted to exposing the truth about the anti-competitive tactics of PBMs
Check out our collection of featured news
Click here for recent articles, video clips, and more!

Watch & learn through helpful videos
Are you a visual learner? Our YouTube channel is a great place to find videos that will help you better understand PBM abuse and other issues currently going on in the pharmacy industry. Our favorites are:
Corrupt Middlemen Are The Real Reason Drug Prices Keep Increasing [February 14th, 2024 | More Perfect Union]
Why CVS Sucks Now—And Is Getting Worse [November 12th, 2024 | More Perfect Union]
Pharmacy Benefit Managers (PBM): America’s Drug Cartel [June 8th, 2024 | UNFTR Media]
Certain videos that aren’t able to be featured on our channel due to YouTube restrictions are listed below for easy reference:
Wisconsin parents lose son because of high cost of medication [March 12th, 2024 | NBC Newswatch 12]
Listen in with podcasts
Do you learn best by listening? Below are a few podcasts or specific episodes we recommend that focus on PBMs and PBM abuse. All are available via the links included as well as several other podcast apps, such as Apple Podcasts, Google Podcasts, Audible, and Spotify.
MTVA Unscripted podcast from Moving to Value Alliance
3-part PBM Problems series (Part 3 features our friend and fellow pharmacy advocate, Luke Slindee!)
On Point podcast from NPR
Pharmacy benefit managers: The middlemen who decide what you pay for medications [12/14/23]
The looming pharmacy crisis in America [12/4/23]
Organized Money | A podcast focusing on “how the business world really works, and how corporate consolidation and monopolies are dominating every sector of our economy”
Episode #3: The Revolt of the Pharmacists Part 1 with Benjamin Jolley [10/23/24]
Episode #4: The Revolt of the Pharmacists Part 2 with Rep. Jake Auchincloss [10/23/24]
PBM on the Rocks from PUTT | A "happy hour style" discussion of PBMs and the effects of their actions across the healthcare spectrum
Want to learn more?
Check us out on social media!
A look at our feed…